MKSAP Quiz: Increasing fatigue for 8 months
A 62-year-old man undergoes a routine examination. He notes increasing fatigue of 8 months' duration but states he can perform his usual daily activities. He has no fever, night sweats, anorexia, or weight loss. The medical history is noncontributory, and he takes no medications.
On physical examination, vital signs are normal. The spleen is palpable three finger breadths below the left midcostal margin. There is no lymphadenopathy or hepatomegaly.
Laboratory studies indicate a hemoglobin level of 12.5 g/dL (125 g/L), a leukocyte count of 14,400/µL (14.4 × 109/L), and a platelet count of 148,000/µL (148 × 109/L).
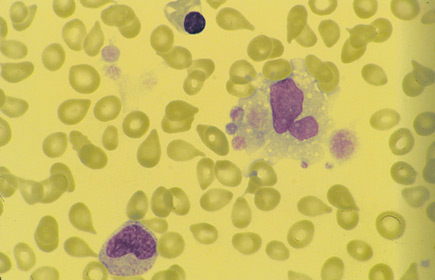
A peripheral blood smear is shown.
The bone marrow cannot be aspirated, but the bone marrow biopsy reveals a hypercellular marrow with extensive fibrosis and abnormal-appearing megakaryocytes. Results of conventional cytogenetic testing are normal. The JAK2 mutation assay is positive. Fluorescence in situ hybridization of the bone marrow for the (9;22) translocation is negative.
Which of the following is the most appropriate management of this patient now?
A. Allogeneic hematopoietic stem cell transplantation
B. Danazol
C. Hydroxyurea
D. Imatinib
E. Observation
Answer and critique
The correct answer is E: Observation. This question can be found in MKSAP 16 in the Hematology and Oncology section, item 1.
The most appropriate management of this patient now is observation. This patient has primary myelofibrosis, which is a chronic myeloproliferative disorder characterized by overproduction of megakaryocytes and bone marrow stromal cell-mediated collagen deposition. The peripheral blood smear shows marked leukoerythroblastic findings with teardrop-shaped erythrocytes and megathrombocytes. The bone marrow aspirate is often “dry” (unsuccessful aspirate), and bone marrow biopsy shows marked fibrosis. This patient has low-risk primary myelofibrosis (PMF) given the absence of high-risk features such as age older than 65 years; fever, night sweats, and a weight loss of 10% or more; a hemoglobin concentration of less than 10 g/dL (100 g/L); a leukocyte count greater than 25,000/µL (25 × 109/L); and circulating blasts of 1% or more. As such, his median overall survival is 135 months or approximately 11 years. Given his favorable prognosis, he requires only observation for now.
Allogeneic hematopoietic stem cell transplantation is potentially curative in patients with PMF but is associated with significant morbidity and mortality and would not be a good choice for a patient with low-risk disease, but it could be considered if the disease progresses. Transplantation is the preferred treatment for younger patients with two or more adverse prognostic features.
Danazol is used to treat PMF-related anemia and leads to responses in 37% of patients with transfusion-dependent anemia or a hemoglobin level less than 10 g/dL (100 g/L). This treatment is not indicated in this patient considering his hemoglobin level of 12.5 g/dL (125 g/L).
Hydroxyurea would be a reasonable therapy if the patient had constitutional symptoms such as fever, weight loss, night sweats, symptomatic splenomegaly, or problematic thrombocytosis; however, this treatment is not required now.
Imatinib is appropriate therapy in patients with chronic myeloid leukemia, but it is not effective in treating PMF.
Key Point
- Close observation, with palliative care as needed, is appropriate for patients with low-risk primary myelofibrosis.



