MKSAP Quiz: Acute onset of fever, chills, cough
A 27-year-old man is evaluated for the acute onset of fever, chills, body aches, and dry cough that began last evening after returning home from trimming timber at a saw mill. He has similar symptoms that have been occurring two to three times a month for the past 3 months. These episodes always occur at home and not at the saw mill but never occur on the weekends or when he is away from home on an extended vacation. Two other colleagues who trim timber at work have also reported similar symptoms over the same time period. His medical history is otherwise unremarkable. He takes no medications.
On physical examination, the patient is currently afebrile, blood pressure is normal, pulse rate is 103/min, and respiration rate is 26/min. Pulmonary examination reveals diffuse crackles throughout all lung zones. Cardiac examination is normal except for tachycardia.
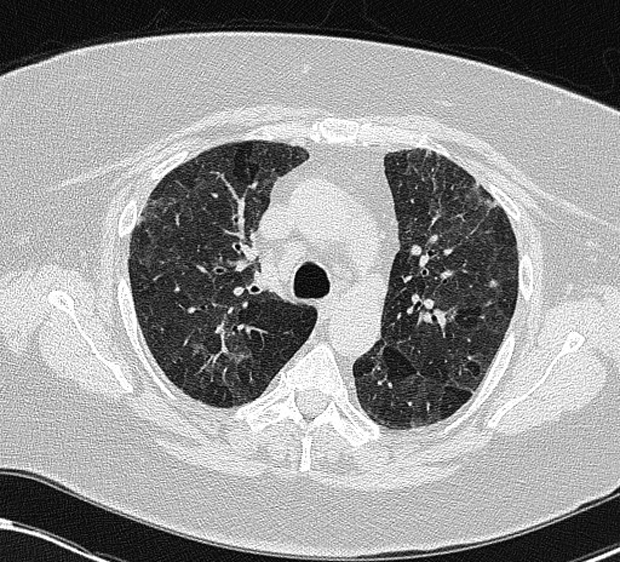
Chest radiograph shows ill-defined haziness in the upper lung zones, but no clear infiltrates. CT of the chest shows mid-lobe–predominant changes; representative findings are shown.
Which of the following is the most likely diagnosis?
A. Acute hypersensitivity pneumonitis
B. Acute interstitial pneumonia
C. Idiopathic pulmonary fibrosis
D. Nonspecific interstitial pneumonia
Answer and critique
The most likely diagnosis is A. Acute hypersensitivity pneumonitis (HP). This question can be found in MKSAP 17 in the Pulmonary and Critical Care Medicine section, item 91.
HP is the result of an immunologic response to repetitive inhalation of antigens. Acute HP presents within 48 hours of a high-level exposure and is often associated with fever, flulike symptoms, cough, and shortness of breath. Radiographic imaging can demonstrate bilateral hazy opacities, and high-resolution CT imaging of the chest shows findings of ground-glass opacities and centrilobular micronodules that are upper- and mid-lobe predominant. Symptoms typically wane within 24 to 48 hours after removal from the exposure. Recurrence of symptoms with exposure to the respiratory antigen is the hallmark of this disorder, and careful attention to the history helps identify the cause. This patient presents with a known or likely exposure to a possible antigen related to his work as a timber trimmer (exposure to agricultural dusts that can readily become colonized with mold), symptoms occurring shortly after possible exposure, a history of similar symptoms, and inspiratory crackles on examination. This constellation of signs and symptoms in conjunction with the radiographic appearance makes HP the most likely diagnosis.
Acute interstitial pneumonia (AIP) is an uncommon form of diffuse lung injury that develops in response to an often unknown insult over a short period of time (days to weeks). Clinically, AIP presents with findings similar to the acute respiratory distress syndrome (ARDS), with severe and progressive hypoxia and imaging showing diffuse bilateral air space opacification. Although the time course of this patient's presentation might be consistent with this diagnosis, his other clinical findings do not support a diagnosis of AIP.
Idiopathic pulmonary fibrosis typically presents in older individuals, and its presentation is more chronic, usually with symptom duration greater than 6 months at the time of presentation. It is therefore not a likely diagnosis in this patient.
Although nonspecific interstitial pneumonia presents in younger patients such as this one, it typically presents as a chronic, rather than acute, process.
Key Point
- Acute hypersensitivity pneumonitis presents within 48 hours of a high-level exposure to respiratory antigens and often is associated with fever, flulike symptoms, cough, and shortness of breath; high-resolution CT imaging of the chest shows findings of ground-glass opacities and centrilobular micronodules that are upper- and mid-lobe predominant.